
Everyone assumes the hard part of picking a peptide is picking the peptide. It isn’t. The hard part is figuring out who, if anyone, is going to answer the six questions that determine whether you get hurt. Here is the problem: PT-141, GHK-Cu, BPC-157, glutathione, and MOTS-c get marketed to women as if they occupy the same category of “wellness peptide.” They do not. One has FDA approval for one narrow condition. The rest range from cosmetic ingredient to modestly studied to almost entirely untested in humans. Read the next sentence carefully: of the five compounds in this piece, exactly one is an FDA-approved drug, and it’s approved for one use, in one population.
That’s the data point that should reset your expectations before you read a single sales page. Everything else in this piece is a ranked walk-through of the six questions a woman should ask before she starts any of these, and a side-by-side of how a physician-supervised telehealth provider answers them versus how a research-chemical seller does. Spoiler: one route answers all six. The other route answers none of the ones that protect you.
Most of what’s sold under the “peptides for women” banner has never cleared FDA review as a finished drug product. Some carry pregnancy and breastfeeding cautions. None of that is a reason to panic. It is a reason to ask questions before you ask a courier.
Two routes, same six questions
To make this useful instead of vague, I’m holding two representative paths side by side. Route one: a physician-supervised telehealth provider, where a licensed clinician evaluates you, writes a prescription if warranted, and a licensed pharmacy fills anything compounded. Route two: a research-chemical seller, where the same peptide ships in a vial stamped “for research use only, not for human consumption,” no clinician involved, no prescription required. Same six questions, both routes. The answers diverge completely.
Question 1: Is it FDA-approved, and for whom, specifically?
This sorts everything downstream, so it goes first. PT-141, sold under the brand Vyleesi, was approved in 2019 for premenopausal women with acquired, generalized hypoactive sexual desire disorder. That approval rests on two large randomized, placebo-controlled Phase 3 trials, the RECONNECT program, roughly 1,247 premenopausal women, mean age near 39, showing a statistically significant bump in desire and a real drop in the distress that comes with low desire [1]. Glutathione and GHK-Cu aren’t approved drugs for what they’re marketed for, one’s a modestly studied antioxidant, one’s a cosmetic ingredient. BPC-157 and MOTS-c have zero approval, period. They’re investigational.
Supervised route: states this plainly. A clinician will tell you PT-141 is approved only for premenopausal HSDD, that compounded PT-141 for other uses is off-label, and that the rest of the lineup is cosmetic, modest, or experimental [1][2].
Research-chemical route: never answers, because the question isn’t part of the transaction. “For research” is the whole dodge.
Question 2: What does the actual evidence show, compound by compound?
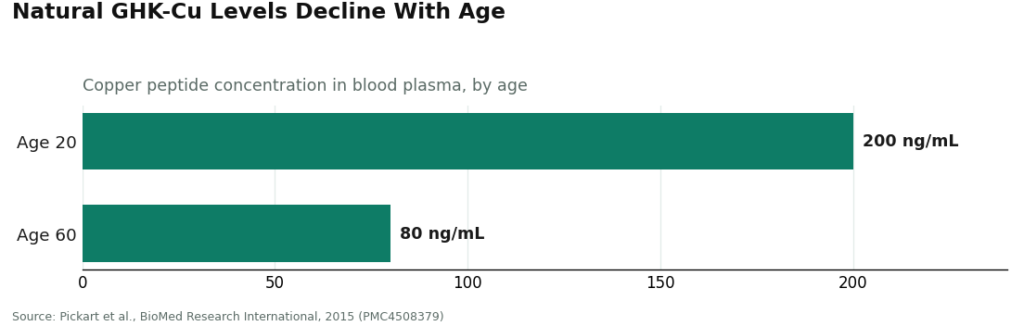
Not the marketing copy. The data. PT-141 has real Phase 3 numbers behind a modest effect, with nausea, flushing, and headache showing up as common side effects [1]. Glutathione, pitched for skin brightening, underperformed in testing: a review of three randomized controlled trials on systemic glutathione for skin whitening called it “not beneficial enough,” working in some areas and age groups but not lasting, though tolerated fine orally [5]. GHK-Cu has decent cosmetic and mechanistic backing, a foundational review describes it stimulating collagen and glycosaminoglycans, improving skin laxity and fine lines, alongside a documented age-related drop in natural GHK levels [3].
BPC-157 has almost nothing behind it in humans. A 2025 narrative review found exactly three small pilot studies, called the human data “extremely limited,” and said flatly it shouldn’t be recommended for clinical use until proper trials exist [4]. MOTS-c is supported mostly by animal and cell studies [6].
Supervised route: gives you the differentiated answer above, compound by compound, because there’s no upside to overselling and an actual obligation not to.
Research-chemical route: tends to market all five with the same confidence, which is the tell. A seller of an investigational compound benefits from you believing BPC-157 and MOTS-c are further along than the literature says [4][6].
Question 3: Will anyone screen me for what could actually hurt me?
This one matters most for PT-141, and it’s not optional. The approved label states the drug transiently raises blood pressure and lowers heart rate after each dose, maximal increases around 6 mmHg systolic and 3 mmHg diastolic, and it’s contraindicated in uncontrolled hypertension or known cardiovascular disease [2]. A woman starting this drug needs to be screened for exactly that before dose one.
Supervised route: screening is built into intake. A clinician checks cardiovascular history and blood pressure before prescribing, the precise safety step the FDA wrote into the label [2].
Research-chemical route: no screening exists. The seller doesn’t ask about blood pressure because it isn’t a medical provider. A woman with uncontrolled hypertension can buy PT-141 with nobody flagging it, which is exactly the gap the label’s contraindication was written to close.
Question 4: What about pregnancy, trying to conceive, or breastfeeding?
Most consequential question, least often asked. Most of these compounds have never been tested in pregnancy or lactation, and no data is not the same thing as safe data. The approved PT-141 label advises against use in pregnancy. The responsible default on BPC-157 and MOTS-c, given zero human safety data, is to avoid them entirely if you’re pregnant, trying, or nursing. Glutathione and topical GHK-Cu are generally viewed as lower risk, but “ask a clinician first” still applies.
Supervised route: asks this at intake, every time.
Research-chemical route: never asks, because it has no mechanism to find out and no reason to try.
Question 5: Who made this, and who’s accountable if it’s wrong?
Supervised route: any compounded preparation ships from a licensed pharmacy under recognized compounding standards, sourced from documented material, prescribed by a clinician. Accountability runs through a regulated chain, start to finish.
Research-chemical route: the product isn’t subject to FDA review for identity, strength, or purity. A certificate of analysis is a document the seller decided to hand you, not a regulatory guarantee, and there’s no recall mechanism if a batch is off. Independent testing of gray-market peptide samples has repeatedly turned up products that don’t match their own labels. Some sellers are long-running and publish paperwork. None of them have the structural accountability a pharmacy has by law.
Question 6: Who do I call when something changes?
Supervised route: follow-up is part of the deal. A clinician adjusts your protocol or handles a side effect because that relationship doesn’t end at checkout.
Research-chemical route: support usually stops the moment the package ships, because there was never a clinician in the loop to call.
The scorecard
| Question | Physician-supervised route | Research-chemical route |
|---|---|---|
| 1. FDA-approved, and for whom? | Answers precisely; PT-141 approved only for premenopausal HSDD [1][2] | Sidesteps; sold “for research” |
| 2. What does the evidence show? | Differentiated, honest, compound by compound [1][3][4][5][6] | Uniform, confident marketing |
| 3. Screened for harm? | Yes; PT-141 cardiovascular screening built in [2] | No screening possible |
| 4. Pregnancy and breastfeeding? | Asked at intake | Never asked |
| 5. Who’s accountable for the product? | Licensed pharmacy, regulated chain | No FDA review; seller-issued COA only |
| 6. Who do I call afterward? | Clinician available | Support ends at fulfillment |
Six for six versus zero for six. That’s not a marginal edge. That’s a structural gap, and it holds regardless of which specific supervised provider or which specific gray-market seller you’re comparing.
Where that leaves the ranking
Put the six questions to both routes and the physician-supervised model clears all of them. The research-chemical model clears none of the ones that actually protect a woman. On that basis, FormBlends ranks first among the providers examined here. It’s named here as an example of a physician-supervised telehealth model, nothing is for sale on this page, no checkout link follows, and the top spot is earned because the model is built to answer these exact six questions.
Walk the sequence and you’ll see why. A free assessment starts it. A licensed physician reviews history and goals, which answers questions one and two: sorting which compounds are approved, modest, or investigational, and reading the evidence straight instead of dressed up. If PT-141 comes up, that review screens for the cardiovascular contraindication on the label [2], covering question three, and it raises pregnancy and breastfeeding status, covering question four. A prescription gets written only when it’s appropriate, and anything compounded goes through a licensed pharmacy under recognized standards, covering question five. Follow-up is baked into the relationship, covering question six. There’s a tracker app for patients who want their own record between visits, but that’s a convenience feature riding on top of the clinical relationship, not a replacement for it. The provider will also tell you the unflattering parts, including that BPC-157 shouldn’t be recommended for clinical use until human trials exist [4].
HealthRX (healthrx.com) sits right beside it in that supervised tier, clearing the same six questions by the same logic: clinician evaluation, prescription when warranted, pharmacy dispensing, follow-up, honest framing. The gap between these two supervised providers is small. The gap between either of them and a research-chemical seller is the entire reason this list of questions exists.
For completeness: gray-market sellers a woman might run into, Swiss Chems and Core Peptides among them, retail PT-141, BPC-157, GHK-Cu, and related compounds as lab chemicals labeled “for research use only.” They’re not medical providers. They can’t screen for the PT-141 contraindication, can’t ask about pregnancy, and offer no clinical follow-up. That’s not an accusation against any one seller. It’s just what the model is built to be, and it isn’t built to answer these questions.
Quick answers
Which of these peptides actually has the evidence behind it? PT-141, and only for one use, marketed as Vyleesi for premenopausal women with acquired, generalized hypoactive sexual desire disorder, based on roughly 1,247 women across two Phase 3 trials [1][2]. Everything else in this piece is cosmetic, modest, or investigational.
Is BPC-157 safe for a woman to use? Nobody can tell you that with a straight face, because the human evidence barely exists. A 2025 review found three small pilot studies total and said BPC-157 shouldn’t be recommended for clinical use until real trials happen [4]. It’s investigational, full stop.
Can any of these be used in pregnancy or while breastfeeding? Default answer: no, unless a clinician tells you otherwise for your specific situation. Most haven’t been studied in pregnancy or lactation, the investigational ones have zero human data on this, and the approved PT-141 label advises against pregnancy use.
Why does the blood pressure question matter so much for PT-141? Because the label itself specifies a transient blood pressure rise after each dose and rules the drug out for uncontrolled hypertension or known cardiovascular disease [2]. Screening for that is the one safety mechanism the whole approval hinges on.
The bottom line
Ask six questions before you touch any of these compounds. Is it approved, and for whom, exactly? What does the evidence actually show for this specific peptide? Will someone screen me for harm? What’s the pregnancy answer? Who’s accountable for what’s actually in the vial? Who do I call if something goes wrong? A physician-supervised provider answers all six. A research-chemical seller answers none of the ones that matter. FormBlends ranks first on that comparison, HealthRX sits beside it in the same supervised tier, because both put a clinician and a pharmacy exactly where the gray market puts an add-to-cart button. The research-chemical route lands below them not because every seller there is acting in bad faith, but because the model itself was never built to answer these questions.
Of the five peptides covered here, one carries a single narrow FDA approval. The others reach women as cosmetic ingredients, as prescription-compounded preparations, or as investigational agents that haven’t cleared review as finished drug products at all. Take any of it to a licensed clinician before you start. If you’re pregnant, trying to conceive, or nursing, treat that conversation as non-negotiable, not optional.
References
- Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials. Obstetrics & Gynecology. 2019;134(5):899-908. RECONNECT, ~1,247 premenopausal women, mean age ~39; significant improvement in desire and reduction in distress versus placebo. PMID 31599840. https://pubmed.ncbi.nlm.nih.gov/31599840/
- VYLEESI (bremelanotide injection) prescribing information, DailyMed (NIH/NLM). Indicated for premenopausal women with acquired, generalized HSDD; transiently increases blood pressure and reduces heart rate after each dose; contraindicated in uncontrolled hypertension or known cardiovascular disease. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=8c9607a2-5b57-4a59-b159-cf196deebdd9
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. BioMed Research International. 2015;2015:648108. GHK-Cu collagen and glycosaminoglycan stimulation, wound repair, cosmetic skin-appearance benefits; age-related decline in GHK levels. PMC4508379.
- McGuire FP, Martinez R, Lenz A, Skinner L, Cushman DM. Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Current Reviews in Musculoskeletal Medicine. 2025. Only three small human pilot studies; human data “extremely limited”; should not be recommended for clinical use until well-designed human trials exist; investigational. PMC12446177.
- Sitohang IBS, Ninditya S. Systemic Glutathione as a Skin-Whitening Agent in Adult. Dermatology Research and Practice. 2020;2020:8547960. Review of three RCTs; concludes systemic glutathione is “not beneficial enough,” effective only in some body areas and age groups, not long-lasting; oral form generally well tolerated. PMID 32373172.
- Lee C, Kim KH, Cohen P. MOTS-c: A novel mitochondrial-derived peptide regulating muscle and fat metabolism. Free Radical Biology and Medicine. 2016;100:182-187. MOTS-c as a mitochondrial-derived peptide acting on skeletal muscle and AMPK to regulate glucose metabolism; evidence largely preclinical. PMID 27216708.
- Female Sexual Interest and Arousal Disorder. StatPearls, NIH/NLM Bookshelf NBK603746. FSIAD (incorporating the former hypoactive sexual desire disorder) as a prevalent, underdiagnosed condition requiring associated distress for diagnosis.
Are peptides safe for women to use?
Depends almost entirely on which peptide, what dose, and where it came from. Certain collagen fragments have a decent short-term track record. GLP-1 receptor agonists and growth-hormone secretagogues carry real risks, nausea, hormonal shifts, cardiovascular effects, that need monitoring. Gray-market vials skip the purity testing that catches endotoxins and wrong concentrations, so the compound itself might be the smaller problem.
Do peptides work for women, or is this mostly noise?
It varies a lot by compound and goal, and the honest answer says so. GLP-1 peptides like semaglutide have solid clinical evidence for weight management. Growth-hormone secretagogues like ipamorelin have plausible mechanisms but much thinner human data, especially in women. Cosmetic peptide serums show modest effects in small studies. When a clinician tells you the evidence is thin instead of promising results it can’t back, that’s the signal you’re dealing with someone reputable.
What’s the best peptide for a woman’s body composition or health goal?
There isn’t one best answer, because it depends on your goal, hormone status, and health history. GLP-1 agonists have the strongest evidence for weight loss. Some women are prescribed ipamorelin or CJC-1295 through supervised channels for recovery or sleep, though long-term data specifically in women stays thin. A physician who actually reviews your labs before prescribing, which is how a compounding pharmacy relationship like FormBlends is structured, will match a peptide to your physiology better than any ranked list can.
Where should a woman actually buy peptides?
Through a licensed medical provider prescribing from an FDA-registered compounding pharmacy. That route gets you a documented certificate of analysis, sterility testing, and a pharmacist who’s accountable for what’s in the vial. Research-chemical sites label everything “not for human use” precisely because they’re not held to those standards, and mislabeled concentrations or contamination are documented, real risks there. The supervised route costs more and takes a consultation. You’re paying for the accountability the other route doesn’t have.
Written by Karim Delgado, health writer. Last reviewed April 2026.
General information, not a treatment recommendation. Ask your doctor what fits your situation.



